70/F RECENT HYPOGLYCEMIA 2°TO ?SEPSIS WITH CKD WITH TYPE 2 DM SINCE 10 YEARS.May 03, 2023
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centred online learning portfolio and your valuable inputs on the comment box is welcome."I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan
CHEIF COMPLAINTS AND HOPI:
A 70 year old female who is a home maker by occupation who is a resident of chityala was brought to the casualty in altered sensorium.
Patient was apparently asymptomatic 10 years back then while doing some work she suddenly lost her consciousness with loss of speech and uprolling of eyes and weakness numbness tingling sensation in right hand and right leg for which they took her to hospital and found having right sided hemiparesis. And after 1 year she had another episode of loss of consciousness and they took her to hospital and got conservative management(like iv fluids) and got discharged.
And now since 3 days she is having 3 episodes of loss of consciousness (one episode per day in the morning) with uprolling of eyes ,protruding of tongue,dribbling of saliva ,and no involuntary movements,no involuntary defecation and micturition,no nausea and vomitings. Patient beacame normal after intake of food and some sugar.
And today morning a similar episode of loss of consciousness at 5:30 they gave sugar to her but her altered sensorium has not resolved and her grbs at home showed to be 7mg/dl (as told by attenders)and was brought to causality in altered sensorium.
she is also having osteoarthritis since 6 years. And she uses volini spray when ever her pain is aggravated.
She got operated for piles 15 years back.
Past history:
Known case of DM2 Since 10years on tablet GLICLAZIDE 30MG AND METFORMIN 500MG PO/OD
K/C/O CVA SINCE 10 years .on RIVOTRIL 0.5 mg PO/OD.
Personal history:
Diet:mixed
Appetite :normal
Bowel and baldder:Regular
Sleep:adequate.
No addictions.
DAILY ROUTINE:
THE PATEINT IS A HOME MAKER BY OCCUPATION SHE DAILY WAKES AT 6AM AND FRESHUP AND DRINKS MILK AND EATS BREAKFAST AND THEN SHE SITS AND CHITCHATS WITH NEIGHBORS WASHES HER CLOTHES AND IN THE AFTER NOON AT 1PM SHE TAKES HER LUNCH WHICH CONSISTING OF RICE AND A VEGETABLE CURRY AND AFTER EATING SHE LIES DOWN FOR SOME TOME AMD WATCHE TV AND DOES SOME HOUSE HOLD WORKS LIKE SWEEPING AND CLEANING HER UTENSILS AND AT 7PM SHE TAKES HER DINNER WHICH CONSISTING OF RICE AND VEGETABLE CURRY. AND SHE WATCH TV FOR SOME TIME AND THEN SLEEPS AT 9PM.
Family history:No similar complaints in the family
She has 2 childern on son and one daughter
Her psychosocial relation ship with her family and neighbors and friends is good.
ON EXAMINATION
PATIENT IS CONSCIOUS
BP:140/70mmhg
PR:84BPM
RR:21CPM
TEMP:AFEBRILE ON TOUCH
GRBS:43mg/DL@ ADMISSION
SYSTEMIC EXAMINATION:
CVS:S1,S2 HEARD,NO MURMURS
CNS: HMF INTACT
NO FOCAL NEUROLOGICAL DEFICITS.
RS:BAE+,NVBS
PA:SOFT AND NONTENDER.
CLINCAL IMAGES:
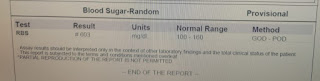
INVESTIGATIONS:
02/05/2023
03/05/2023
PROVISIONAL DIAGNOSIS:
RECENT HYPOGLYCEMIA 2°TO ?SEPSIS WITH CKD WITH TYPE 2 DM SINCE 10 YEARS.
TREATMENT
IVF :DNS 75ML/HR
INJ:MONOCEF 1gm IV/BD(D2)
TAB:CLONAZEPAM 0.5gm PO/OD
TAB:SODIUM VALPORATE 300MGPO/OD
TAB:ECOSPIRIN 75/10 PO/HS 9PM
MONITORING VITALS HOURLY.
:::::::::::::::: FOLLOW UP::::::::::::
03/05/2023
S:
2 FEVER SINCE ADMISSION
STOOLS NOT PASSED.
O:
ON EXAMINATION
PATEINT CONSCIOUS,COHERENT,COOPERATIVE.
BP:140/60mmhg
PR:74 BPM
RR:21CPM
TEMP:96.7°F
GRBS:183mg/dl @10AM
CVS:S1 S2 HEARD AND NO MURMURS
RS:BAE PRESENT.NVBS HEARD
PA:SOFT AND NONTENDER
CNS:HMF-INTACT
NO FOCAL NEUROLOGICAL DEFICITS.
A:
RECENT HYPOGLYCEMIA 2°TO ?SEPSIS WITH CKD WITH TYPE 2 DM SINCE 10 YEARS.
P:
IVF :DNS 75ML/HR
INJ:MONOCEF 1gm IV/BD(D2)
TAB:CLONAZEPAM 0.5gm PO/OD
TAB:SODIUM VALPORATE 300MGPO/OD
TAB:ECOSPIRIN 75/10 PO/HS 9PM
MONITORING VITALS HOURLY.
QUESTIONS DURING THE ROUNDS:::
REASON FOR HER HYPOGLYCEMIA??
May be? kidney failure...
DURING ROUNDS SIR ASKED HER TO SHOW HOW TO LOAD INSULIN AND HOW TO INJECT IT BUT THE PATIENT DUE TO HER WEAKNESS IN HER RIGHT HAND NOT ABLE TO HOLD THE VIAL .SO WE EXPLAINED THE PATIENT ATTNEDER HOW TO LOAD AND HOW TO INJECT.
SUMMARY::
Diagnosis....
Diabetes mellitus type 2 since 10 years
Hypoglycaemic attacks since 3 days (3 episodes ,1 episode per day)
HISTORY:
A 70 YEAR OLD FEMALE WHO IS A RESIDENT OF TELANGANA KNOWN CASE OF DIABETES SINCE 10 YEARS,CVA SINCE 10 YEARS HAVING HYPOGLYCEMIC ATTACKS SINCE 3 DAYS
ON EXAMINATION
PATIENT IS CONSCIOUS
BP:140/70mmhg
PR:84BPM
RR:21CPM
TEMP:AFEBRILE ON TOUCH
GRBS:43mg/DL@ ADMISSION
SYSTEMIC EXAMINATION:
CVS:S1,S2 HEARD,NO MURMURS
CNS: HMF INTACT
NO FOCAL NEUROLOGICAL DEFICITS.
RS:BAE+,NVBS
PA:SOFT AND NONTENDER.
COURSE IN THE HOSPITAL...
PATIENT WAS GIVEN DEXTROSE NORMAL SALINE AFTER ADMISSION AND HER CONSCIOUSNESS HAS BEEN IMPROVED.
INVESTIGATING FOR THE REASON FOR HER HYPOGLYCEMIA..